
Unenhanced Helical CT
In The Patient With
Acute Flank Pain
Mindy M. Horrow, MD, FACR
Director of Body Imaging
Albert Einstein Medical Center
Clinical Associate Professor of Radiology
Jefferson Medical College
Thomas Jefferson University
All photos retain the copyrights of their original authors
© Mindy Horrow, MD
Background
•Over a lifetime, approximately 2.3% of thepopulation will have an episode of acuterenal colic
•All calculi, regardless of composition willhave attenuation values (200-600 HU)greater than surrounding soft tissues
•Multi-slice helical CT allows thin sectionsand reconstructions to reduce volumeaveraging effects and better demonstratehigh attenuation of a calculus
Comparison of Non-Enhanced CTand Intravenous Urography
•20 patients with both studies
•12 had ureteric obstruction on both studies
–5 had demonstrable ureteric stone onboth
–6 had stone seen only on CT
–1 had no stone seen on either study
•8 without obstruction on either study
Smith et al: Radiology 194:789, 1995
Results
•Studied 292 patients, with confirmation of CTdiagnosis in 210
•100 patients had confirmed ureteral stones onother studies
•110 patients had confirmation of no stones
•30 patients with other diagnoses (adnexalmasses, appendicitis, diverticulitis, commonbile duct stones)
•CT false negative in 3, false positive in 4
•Sensitivity 97%, Specificity 96%, Accuracy 97%
Smith et al AJR 166:97, 1996
AEMC Study
•Between April 1995 and April 1997,412 consecutive patients
•281/412 had confirmation of CTdiagnosis by other radiologicimaging, urologic intervention,spontaneous passage of stone
Nachman, et al Am J EmergMed 18:649, 2000
AEMC Results
•Positive for calculi 33% (92/281)
•Negative for calculi 67% (189/281)
•Other diagnoses in 189 pts32%(60/189)
•Sensitivity97%
•Specificity 92%
•Positive predictive value 88%
•Negative predictive value 98%
Protocol
•5 mm slices
•Save raw data forreconstructions as necessary(reconstruct to 2.5 mm)
•No oral or intravenous contrastinitially. Use only in problemcases.
Primary Findings
•Calcific density in ureter,uretero-vesical junctionor bladder
Secondary Findings
•Ureteral dilatation
•Collecting system dilatation
•Perinephric stranding
•Renal enlargement
•Renal hypodensity


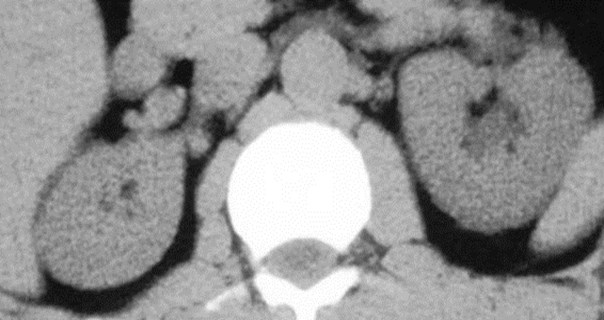
Right Flank Pain


Left Flank Pain
Secondary Signs of AcuteUreteral Obstruction
Secondary SignSensitivitySpecificityAccuracy
Ureteraldilatation90 (82-95)93 (86-97)91 (86-94)
Perinephricstranding82 (73-89)93 (86-97)87 (82-91)
Collecting systemdilatation83 (74-89)94 (87-98)88 (83-92)
Nephromegaly71 (61-69)89 (81-94)80 (74-85)
Smith et al: AJR 167:1109, 1996
Secondary Signs
•Unilateral ureteral dilatation ANDperinephric stranding had positivepredictive value of 99%(86 or 87 patients)
•Absence of ureteral dilatationAND perinephric stranding had anegative predictive value of 95%(5/109 patients)
Ureteral Stone Disease Present If:
•Calcific density in ureter, uretero-vesical junction or bladder
•Unilateral ureteral dilatation andperinephric stranding (or othersecondary findings) onsymptomatic side withoutdemonstrable calculus
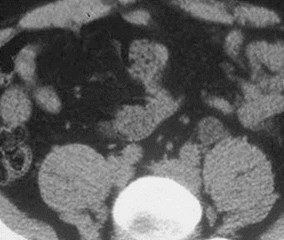
Left Flank Pain






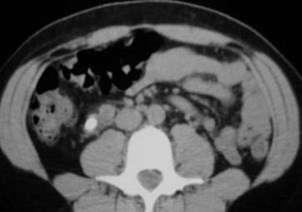
Patient with right flank pain andmild right hydroureteronephrosis

Right ureteral calculus passed into bladder

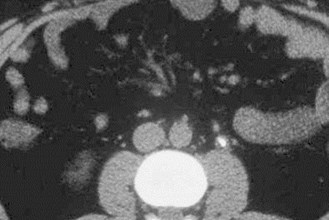
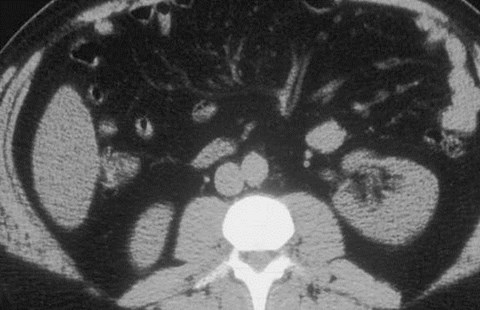
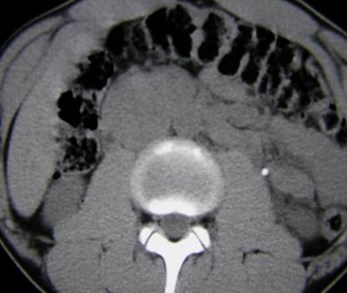
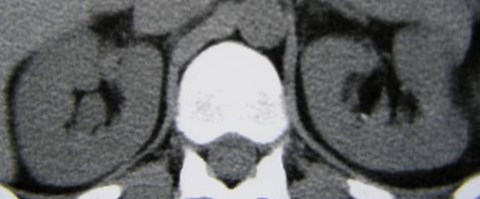
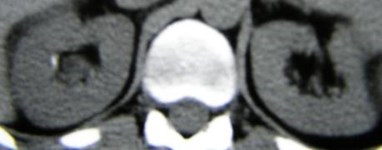
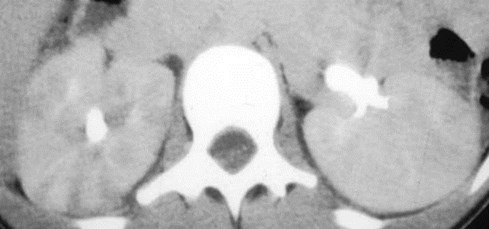
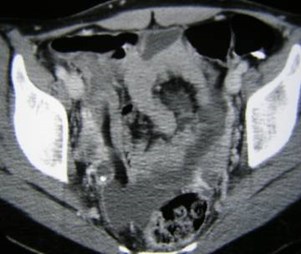
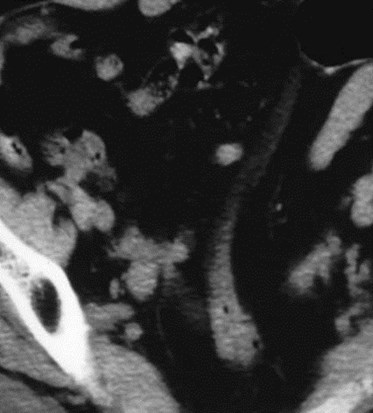
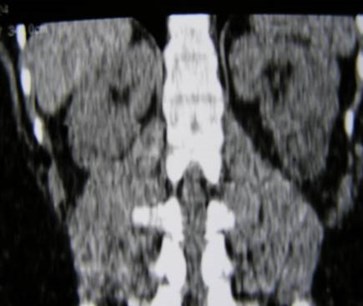
Right flank pain
Enlarged, hypodense right kidney
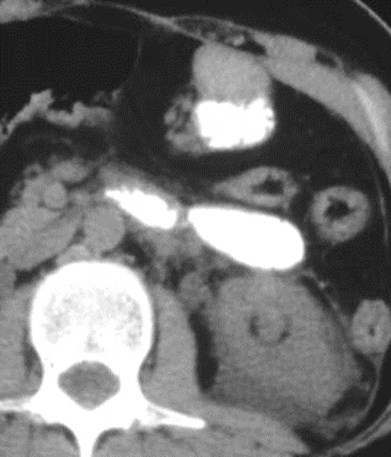
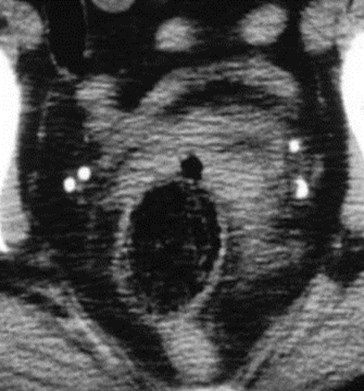
Right UVJ Calculus

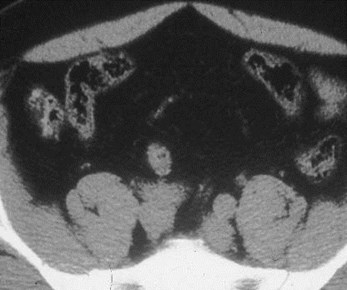
Left flank pain

Which calcification is the calculus?


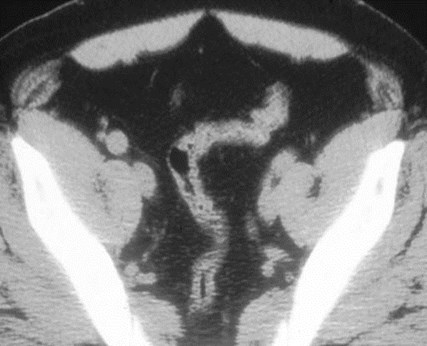
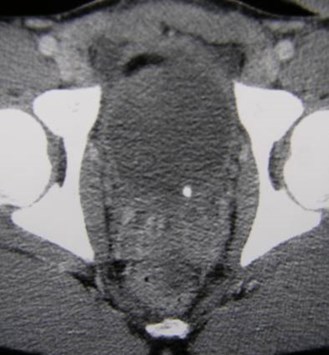
CT scan 6 hours later
Calculus has passed into bladder

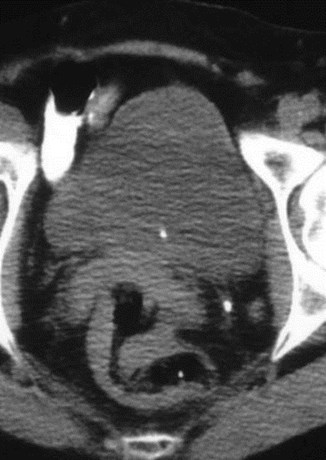
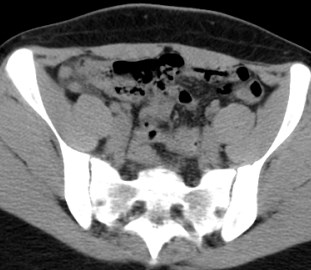
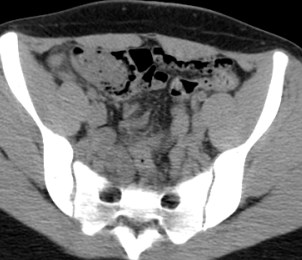
Acute Left Flank Pain
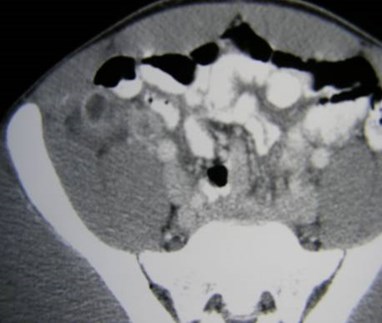
Patient returns 2 months laterwith right lower quadrant pain
Appendicitis with calculus in bladder


Re-examination one day later
Stone passed and perinephric fluid resolved



Right flank pain in patient with right stent
Acute left flank pain



R

How many calculi do you see?




1mm re-indexed images
There are atleast 5 calculi
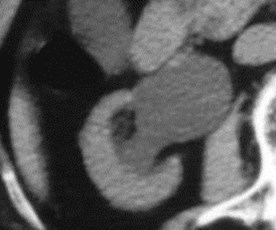
Calculi vs. Phleboliths
Geometric configuration21%0%
Central lucency0%9%
Bifid peak0%21%
“Comet Sign”0%21%
Soft tissue rim sign76%8%
Mean attenuation305 HU160 HU
(No phleboliths had mean attenuation greater than 278HU )
Bell et al: Radiology 207:363, 1998
Heneghan et al: Radiology 202:709, 1997

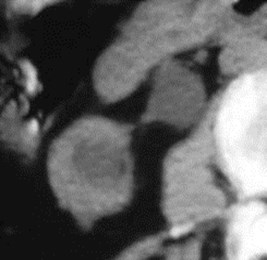
Soft Tissue Rim Sign

Which side is painful?
Which is the calculus?
Irregular shape, soft tissue rim
Low density center of a phlebolith

Comet tail sign
Attenuation Differencebetween Kidneys
•Attenuation differences betweenkidneys were higher for patients withureterolithiasis: 5.43.2 H (range –3.3to 13) versus 1.2 1.0 H (range 0- 4.7)
•Attenuation difference betweenkidneys 5.0 H had 61% sensitivity,100% specificity, 100% PPV, 69% NPVand 79% accuracy
Goldman, et al. AJR182:1251, 2004

Right flank pain

RUVJ Stone
Detection of Ureteral CalculiPlain Radiography vs. Unenhanced Helical CT
•CT detects virtually all calculiregardless of composition
•Plain radiographs had sensitivity of59%
Levine et al: Radiology 204:27-31,1997
Improving Detection ofCalculi on AbdominalRadiographs
•In study of 58 patients with ureteralstones on CT, abdominal radiographsdetected
–45% when viewed alone
–66% when viewed with axial CT scan
–78% when viewed with axial CT and MIPimages
Better use of plain films for lithotripsy, and to follow stonepassage.
Van Beers, et al AJR 177:1117, 2001
Non-opaque Calculi on CT
•6 HIV patients receiving protease inhibitortherapy with Indinavir reported to haveureteral obstruction from deposition ofcrystals which are not radio-opaque
•May require IVU or retrograde urographyto establish diagnosis
Blake, et al. AJR 172:1452, 1998
Relationship of Spontaneous StonePassage of Size and Location
•Spontaneous passage rate for calculi:
–1-4 mm, 78%
–5-7 mm, 60%
– 8 mm, 39% p<0.001
•Frequency of spontaneous stonepassage only significant comparingproximal ureter (48% passage) andureterovesical junction (79% passage)
Coll, et al AJR 178:101, 2002
Extent of Perinephric Edema andDegree of Obstruction
•47 patients with acute ureterolithiasis onunenhanced CT had excretory urography
–8 without stranding on CT had non-obstructingcalculi on IVU
–21 with limited edema at CT had low gradeobstruction on IVU
–15 with extensive edema at CT had high gradeobstruction at IVU
–3 with extensive edema at CT had low gradeobstruction at IVU
•Extent of edema allowed accurate prediction ofdegree of ureteral obstruction in 44 (94%)
Boridy et al Radiology 213:663, 1999
Does Extent of Secondary Signscorrelate with Clinical Situation?
•Duration of flank pain determined prospectivelyin 227 patients with acute ureterolithiasis onunenhanced CT
•Frequency of:
–Ureteral dilatation from 84% at 1-2 hr to 97% at 8 hr(p<0.03)
–Collecting system dilatation from 68% at 1-2 hr to89% at 7-8 hr (p<0.03)
–Moderate or severe stranding from 5% at 1-2 hr to51% at 7-8 hr (p<0.001)
–Moderate or severe perinephric fluid from 0% at 1-2 hr to 22% at 3-4 hr (p<0.03)
Varanelli, et al AJR 177:325, 2001
Relationship of StoneAttenuation to LithotripsyOutcome
•Study of 30 patients with calculi , 20 mm
•Success rate for stones > 1000 H wassignificantly lower than for stones < 1000H(6 of 11 versus 18 of 19 cases, p<0.01)
•Stones > 1000 H required greater number ofshock waves for fragmentation
Joseph, et al J Urol 167:1968, 2002
Unenhanced CT vs.. Ultrasound
•Unenhanced CT has higher sensitivity fordetection of ureteral calculi than US (96 vs. 61%)
•Unenhanced CT has higher sensitivity for ureteralcalculi compared to combination of US and plainradiography (92 vs. 77%)
•Calculi missed by the combination technique weresmall and passed spontaneously.
•Therefore the US plain film combination is analternative when CT is not available or indicated.
Catalano, AJR 178:379, 2002
Sheafor, Radiology 217:792, 2000


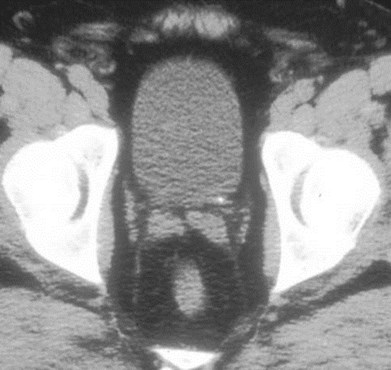
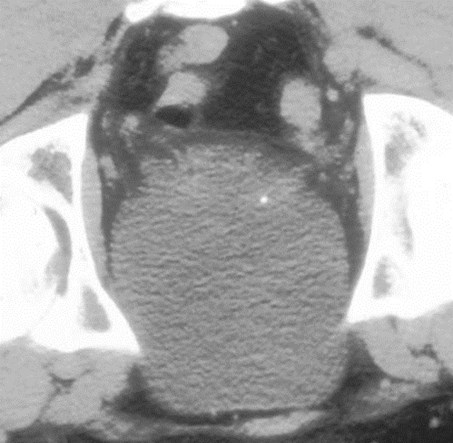
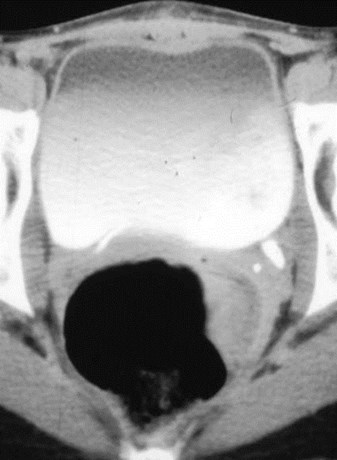
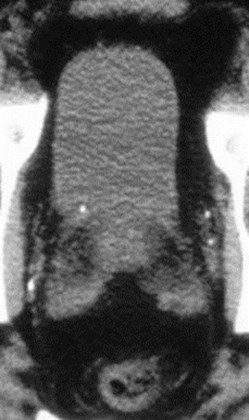
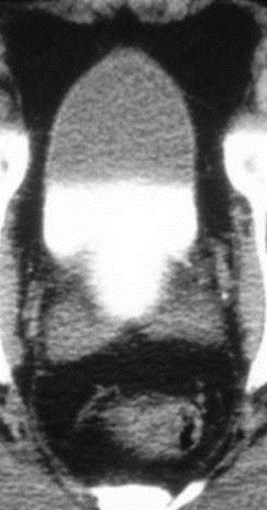
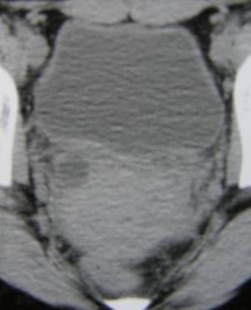
Bladder
Right Flank pain
Distal right ureteralcalculus with absent “jet”

Left flank pain

6 months earlier

Right kidney
Left kidney



Confirms distal left ureteral calculus
Other Diagnoses
•Diverticulitis
•Appendicitis
•Pyelonephritis
•Pancreatitis
•Ovarian Masses
•Other: ingested needle, stomachcarcinoma, ruptured aorticaneurysm
•Other urinary tract abnormalities
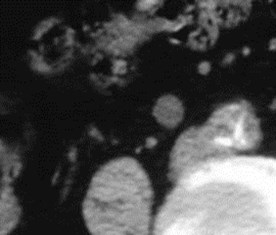
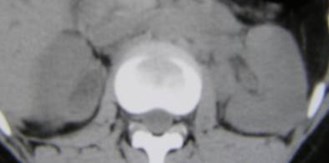
Left sided flank pain

What is your diagnosis?
IV contrast, delayed imaging
URETER
PHLEBOLITH
Pyelonephritis

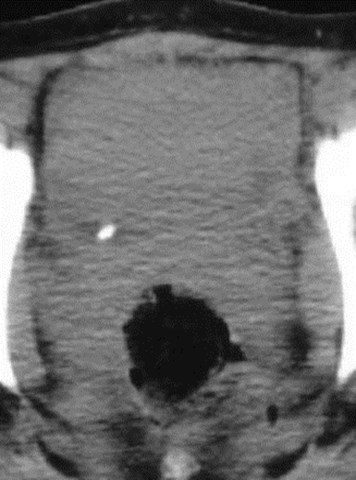
Right Flank Pain

Pyelonephritis anddistal right ureteralcalculus in patientwith a V-P Shunt

Right sided flank pain


Renal cellcarcinoma andureterolithiasis
Right flank pain

Transitional cell carcinoma


1997
1995
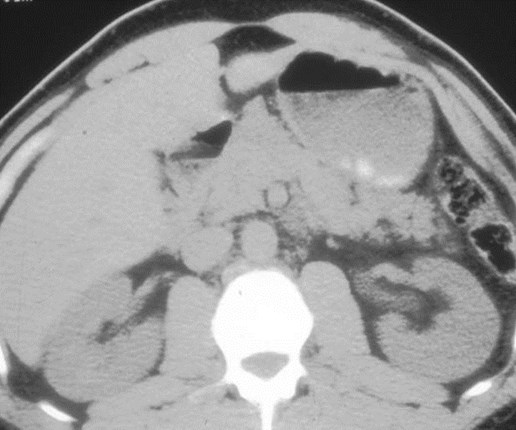
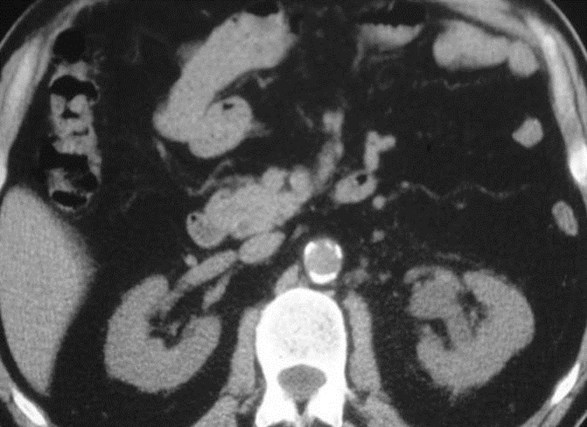
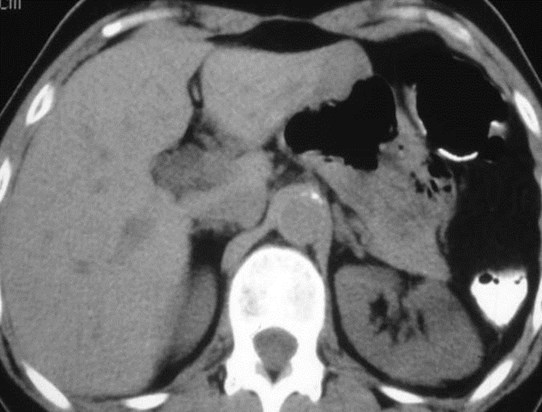
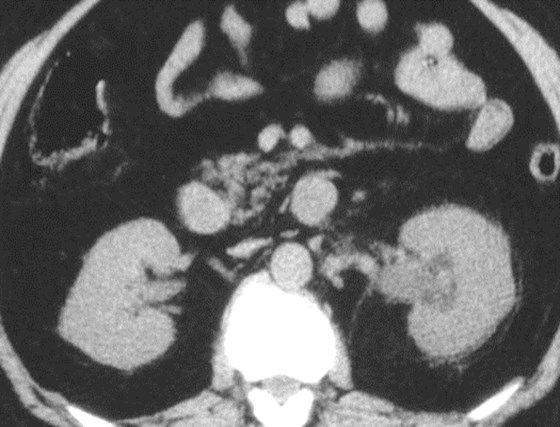
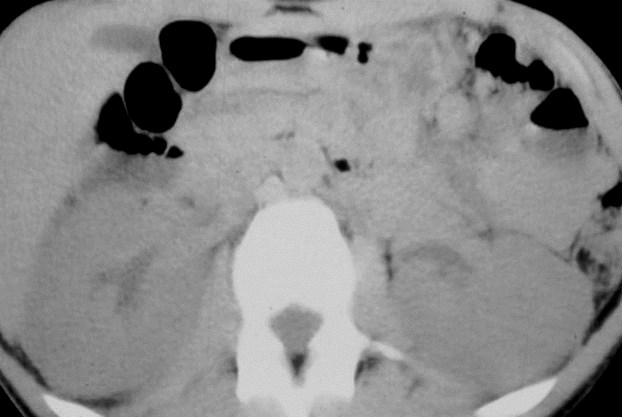
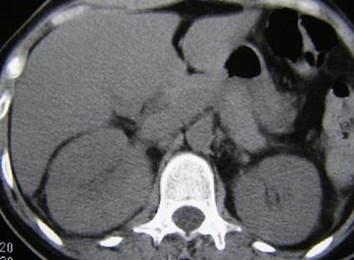
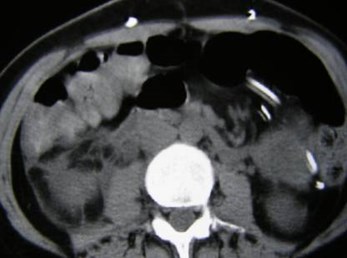
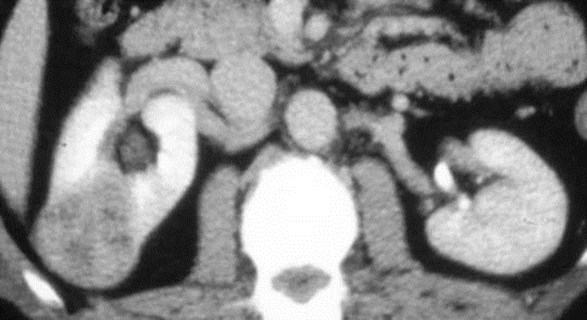
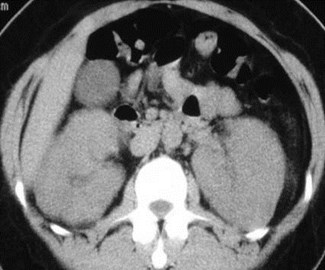
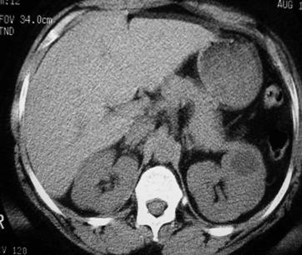
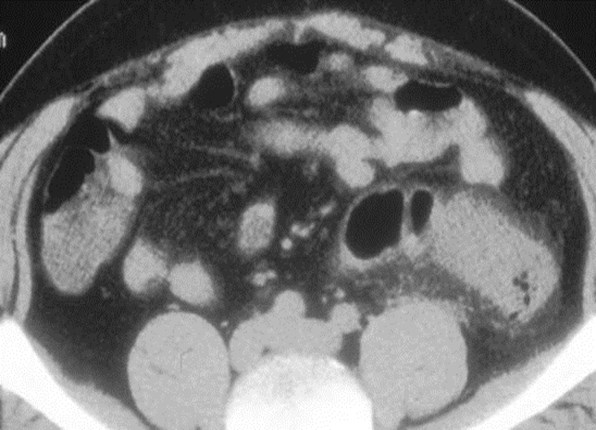
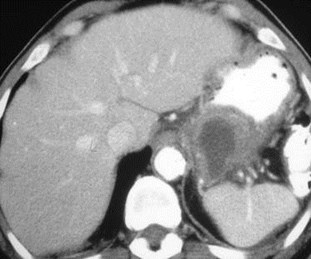
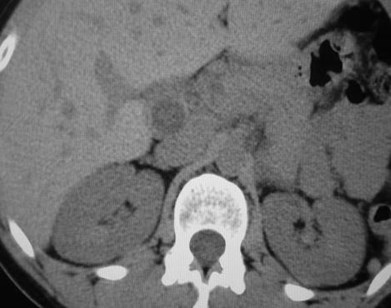
Patient with CML inBlast Crisis:splenomegaly andnephromegaly


Right flank pain
1.Acute R ureteralcalculus
2.Hepatosplenomegaly
3.Lymphadenopathy
4.Renal calculi
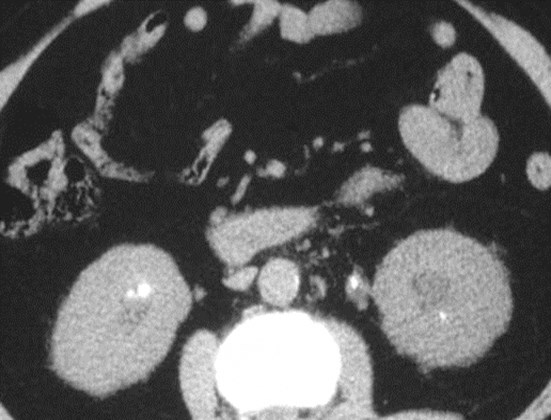
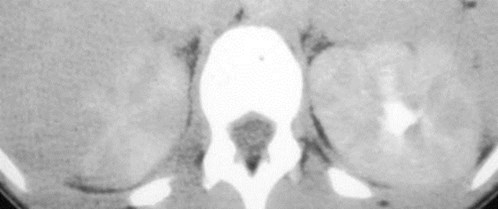
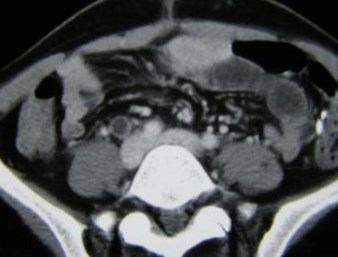
Sarcoidosis



Left Flank Pain

Bifid collecting system with chronicobstruction of lower pole moiety

Confirmation of CT findings with retrograde study




Chronic obstruction of upper pole moiety ofa duplicated kidney
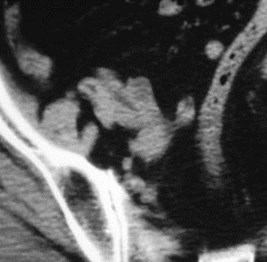
Left flank pain
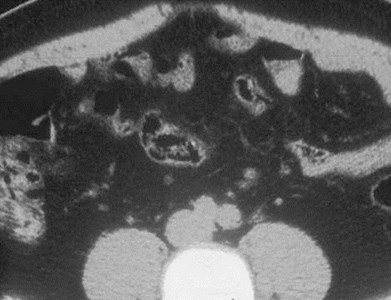
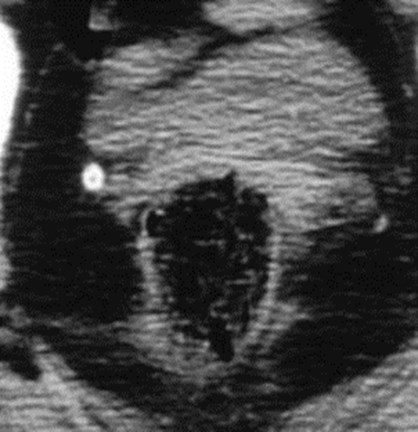
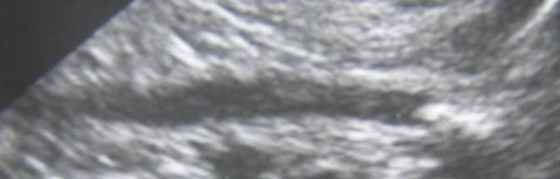
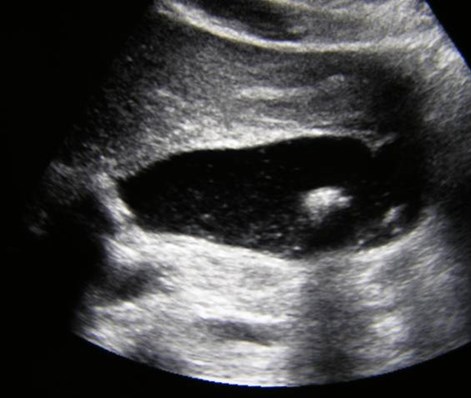
Diverticulitis


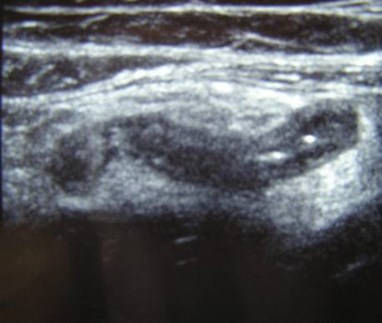

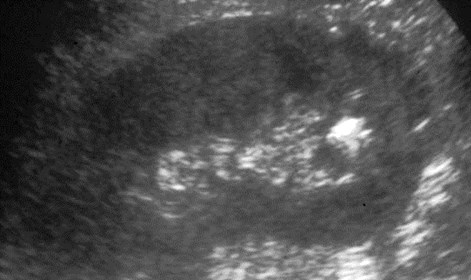
Blind ending, non-compressible tubularstructure, 7mm thickness, adjacentechogenic fat indicating inflammation
Appendicitis



Left flank pain
Pancreatitis with pseudocyst

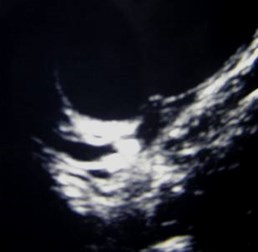
Right Flank Pain
Sonographic Murphy Sign, sludge, calculi, fluid
Acute Calculus Cholecystitis

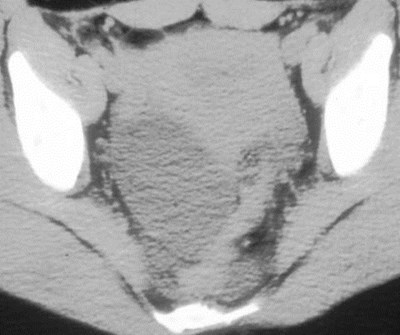
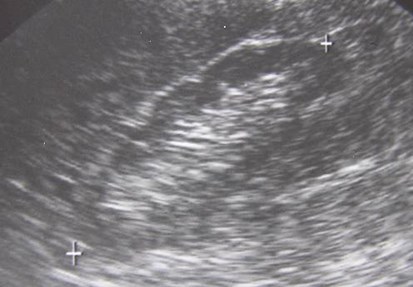
Two female patients with right flank pain
Dermoid
Ovarian cyst
Algorithm
•Definite ureteral calculus:
–No further imaging
•No ureteral calculus or 2 signs:
–Ureteral stone diseaseexcluded
–Look for alternate diagnosis
Algorithm
•No ureteral calculus, but ureteral dilatation andperinephric stranding on symptomatic side:
–Most likely recent stone passed or very smallureteral stone
–However, if fever and wbc, considerpyelonephritis
•One or more 2 signs on symptomatic side andsuspicious calcification:
–If “rim sign,” probably ureteral calculus
–Otherwise, calcification is indeterminate
The End